

Specific research has been conducted around the different ways of female heart arterial disease. This is a landmark study of life or death significance.Have Dozens of scientific articles1 Solve this topic.
Different symptom patterns
In all American medicine, there is no better example than women with heart disease to illustrate the disconnect between what we know and what we do. Although the different symptom patterns of women with abnormal heart arteries are receiving more and more attention, failure to translate these best practice treatments can make their lives more dangerous and expensive. Women presenting to the emergency room with chest pain or other symptoms suggestive of coronary artery disease will be evaluated according to an outdated scientific paradigm aimed at finding blocked arteries. She will undergo a stress test and/or cardiac catheterization. If these tests are normal, the patient will be told that these symptoms have nothing to do with her heart. I saw patients with repeated chest pains and was told that the problem was in the esophagus or more severe depression. She was actually told: “Go home, bring your stability and Prozac, and you will be fine!” What she was told was wrong—often very wrong!
U.S. taxpayers have paid for a specific study on the unique nature of coronary artery disease in women.Survey results NIH sponsored WISE research2 (Assessment of Female Ischemic Syndrome) Research is extremely important and has very practical significance.
Gender differences
Coronary artery disease in women is different from coronary artery disease in men. This disease in men can cause local arterial blockage and chest pain during exercise, which can be relieved after rest. Many women develop cholesterol deposits that are evenly distributed throughout the arterial system, resulting in smaller arteries that are less locally blocked. Nonetheless, these deposits can still crack and produce clots. Most heart attacks are coagulation events, which explains why the anticoagulant aspirin can prevent heart attacks, while anticoagulants prevent heart attacks that are already ongoing. When a clot blocks an artery, it kills the downstream heart muscle and causes a heart attack.
related information: Heart attack: when will we finally do what needs to be done?
Not only are cholesterol deposits prevalent in women, but also push3 The arterial wall faces outwards, so it can be very large before any blockage occurs.These soft, inflamed, and dangerous deposits explain why women with recurrent chest pain in the WISE study still have high risk4 Heart attack and sudden death, even with normal cardiac catheterization. What these women really need is the best drug treatment for their vascular risks, which has been shown to have a powerful effect on stabilizing cholesterol deposits, relieving symptoms, and preventing heart attacks. The best medications include aspirin, blood pressure control, cholesterol management, and smoking cessation. Patients with diabetes and prediabetes should take metformin.Female patients who already have chest pain may benefit from beta blockers, nitroglycerin and new drugs such as Lanesa.5 70% of these women can completely relieve chest pain within one year after receiving the best medical treatment.
Diagnose the error?
Our current medical system continues to operate in a fixed occlusion mode for coronary artery disease. If the patient has no fixed obstruction, they will be told that the problem has nothing to do with the heart. What are the consequences of this diagnostic error?
The real problems of these women have not been effectively resolved. One year after undergoing catheterization, only about 10% of these women received any treatment for blood pressure and cholesterol problems. Many women with recurrent chest pain continue to suffer unnecessary pain and torture. Many of them had a heart attack, and too many died. Personal costs are devastating. Since the real problem has not been resolved, these women often return to the emergency room for repeated examinations and hospitalizations, and seek a second opinion.this Lifetime cost 6The cost of care for women with recurrent chest pain and no heart artery blockage is close to US$800,000. These women need the best treatment, and they respond well to it. I have treated about 25 women like this, and they are the most grateful patients I have ever helped. Medication relieved their pain and made them safer.
Calculate your risk of heart attack
If you are a woman 69 years of age or older, your risk of heart attack will increase. Even if your cholesterol is not elevated and there are no other risk factors, you should take statins. Use the link above to calculate your heart attack risk, if it exceeds 7.5%, then you need the best treatment for heart artery disease. Age is the most effective heart risk factor.About half of deaths are caused by heart disease happen suddenly7 And there are no warnings. These women have no chance to protect themselves. If you know a woman with a family history of heart disease, or a woman age 69 or older, or a woman with recurrent chest pain, please recommend this article to them. It’s time to take more seriously the unique needs of female patients with heart disease. When will we stand up and protect our mothers, wives and neighbors?
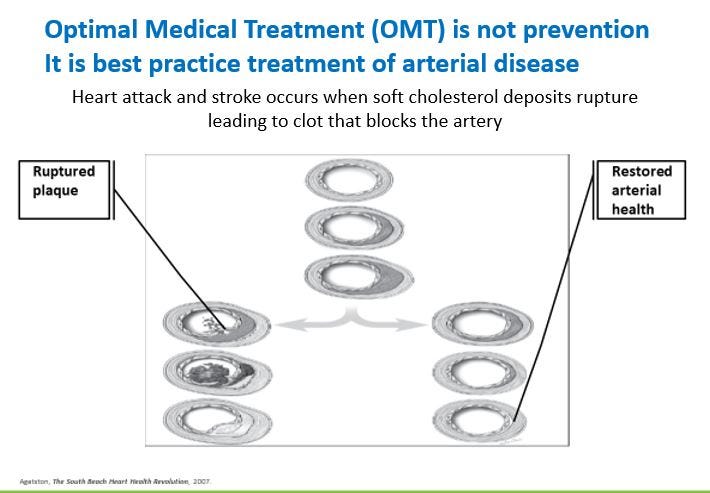
These pictures represent heart arteries that have been severed like garden hoses or soda straws. Start at the top of the picture. That is a normal artery. The next picture has a dark gray cholesterol deposit extending from about 1 o’clock to 6 o’clock. Below it is a larger deposit, which is soft, inflamed, and easily ruptured, but still completely unblocked the artery. This is why women without obstruction may have a heart attack.
On the left, you can see what happens to patients who have not received the best treatment. As shown in the first picture, cholesterol deposits may break. This causes the clot you see in the second picture, and then the scar tissue you see in the third picture to form and block.
On the right, you will see the best medical (OMT) results. Cholesterol deposits stabilize, inflammation is reduced, and it is much less likely to rupture and cause a clot to cause a heart attack. These changes can provide you with more protection in a few days. As you can see, medication can reduce these soft and dangerous deposits and make the arteries more normal. We now have a much better understanding of heart artery disease, and there are very targeted and precise treatments that can protect you. This image is from the South Beach Heart Health Revolution and I used it with the permission of Dr. Agaston.
This is new information, and I know some of you must have questions, if you put them in the comments, I will be happy to answer them. I believe this information will save lives, and I hope you can tell your friends.
refer to
- The female ischemic syndrome was evaluated by the National Institutes of Health. https://www.ncbi.nlm.nih.gov/pmc/?term=This+Women%27s+ischemia+syndrome+assessment
- The WISE study of women and heart disease yields important findings on the often undiagnosed coronary syndrome. National Institutes of Health. Press release, January 2006.
- Matheen A. Khuddus, MD, Carl J. Pepine, MD, Eileen M. Handberg, Ph.D., et al. Intravascular ultrasound analysis of women experiencing chest pain without obstructive coronary artery disease http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3019081/pdf/nihms259264.pdf
- B. Delia Johnson1, Leslee J. Shaw, Carl J. Pepine, Steven E. Reis, etc., persistent chest pain can predict cardiovascular events in women without obstructive coronary artery disease: NIH-NHLBI-sponsored evaluation of female ischemic syndrome ( The result of WISE) learning. European Heart Journal 2006. http://eurheartj.oxfordjournals.org/content/27/12/1408.full.pdf
- S. Ndegwa, Ranolazine (Ranexa) for the treatment of chronic stable angina pectoris, National Library of Medicine, Issue Emerge Health Technol. June 2007; (99): 1-6. https://pubmed.ncbi.nlm.nih.gov/17595750/
- Leslee J. Shaw, PhD; C. Noel Bairey Merz, MD; Carl J. Pepine, MD; etc., The economic burden of angina pectoris in women with suspected ischemic heart disease
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0000342/ - Puja K. Mehta, MD; B. Dr. Delia Johnson; Dr. Tanya S. Kenkre and others, Sudden cardiac death in women suspected of ischemic heart disease,
William H. Bestermann, Jr., MD
William H. Bestermann Jr., MD He is a board-certified physician and has been engaged in preventive cardiology for more than 20 years. His core expertise is to consistently provide optimal medical treatment (OMT) for cardiovascular and related diseases. He does this by using evidence-based care processes consistent with best practices.
He sees OMT as a product. He understands how healthcare organizations combine new systems, new science, and new payment models to produce the product more consistently. This combination can be standardized, scaled and industrialized. These new systems combine teams, protocols, population health tools, clinical/financial analysis, and provider training. Certain clinical interventions reduce clinical events than they have a greater impact on target risk factors.
Dr. Bestermann has developed a comprehensive program that combines these interventions to minimize weight loss, minimize drug interactions, and reduce side effects. When these systemic interventions are used in combination, they can significantly reduce the cost of care, prolong life and delay cardiovascular events.
Dr. Bestermann wrote the first article on metabolic syndrome systems and comprehensive methods. He later collaborated with many academics and community leaders to write a more detailed article on the science and treatment of metabolic syndrome. He proposed a new mechanism of action of metformin and explained its effects on cardiovascular, events, cancer and aging.
He oversaw an advanced medical family team within Holston Medical Group responsible for the treatment of cardiometabolic diseases, including PharmD’s outpatient care resident. The team manages Eastman Chemical Company’s high-risk diabetes and high blood pressure employees.
He is also a senior clinical consultant for the Quality Blue Primary Care Program in BCBS, Louisiana. This effort has reduced hospitalizations, hospital stays, and specialist referrals, while reducing monthly expenses for each member. He has personal experience producing OMT in multiple medical environments.
He has been convinced that only evidence, data, and transparency can free us from the low-value health care that prevails in the United States. There are many vendors claiming their clinical and financial success. Most of these statements are invalid. Few people consistently apply the best medications to patients suffering from cardiovascular diseases and related diseases in a way that prolongs life, delays cardiovascular events, and reduces costs.Dr. Bestman submitted his method Verification Agency And got their seal of approval.
In addition to being a contributing author of The Doctor Weighs In, Dr. Besterman also serves on the TDWI Editorial Board, where he conducts medical reviews of articles submitted for publication.



{kind=link}