

Pain
Conceptually, over our lifetime we all gain some understanding and insights into pain. But for a person living with chronic pain, it can seem as if the world doesn’t understand.
And the truth is, sometimes the world doesn’t understand.
Even for medical professionals, whose primary role is to provide care, chronic pain can be difficult to appreciate. Because chronic pain is measured subjectively and not well understood, physicians historically viewed chronic pain as a characterological flaw rather than a “true” disease. While we have come a long way in understanding chronic pain states from a pathophysiologic basis, we still have a long way to go. A person’s socioeconomic status, race, ethnicity and gender may disproportionally expose them to this historical bias in viewing their pain as more “psychosomatic” or less legitimate, thereby subjecting them to disparities in receiving appropriate pain care.
We know, for example, that racial and ethnic minorities are less likely to receive adequate treatment for both acute and chronic pain than their white counterparts, even after controlling for variables, such as age, gender and intensity of pain.[1] And when looking at gender, we find that women’s pain is more likely to be downplayed by healthcare—even in the literature—because there is a perception that women are more sensitive to pain or that they are more likely to report pain when compared to men.[2]
When pain isn’t taken seriously, then people don’t get the care they need to address it. Nowhere is this more evident than in interventional pain care, where therapies, such as spinal cord stimulation, dorsal root ganglion and radiofrequency ablation, are underutilized relative to how long these types of therapies have been available and the number of patients who could benefit from them. But simply trying to increase the number or access to interventional procedures isn’t the answer. Instead, we need to understand the barriers that exist and address them accordingly.
The Physician Factor
One of the first areas to look is to the healthcare system itself. Within it, we see that both minorities and women are vastly underrepresented in medicine, in general, and in interventional pain medicine specialties, despite recent advancements that have been made on this front. Consider for a moment that in 2018, only 5% of all doctors were African American or black[3] even though they make up more than 13% of the U.S. population[4]. When looking at interventional pain medicine specialties, the numbers were even lower, with African Americans or black people making up just 4.7% and 3.8% of anesthesiologists and neurosurgeons, respectively.[5], [6] The number rises slightly in the pain medicine specialty, where African American or black doctors make up 5.9% overall.[7], [8] Only by further segmenting the specialties and looking at gender, as well as racial demographics, can we find a double-digit representation—10.3% of all female pain medicine specialists are African American or black.
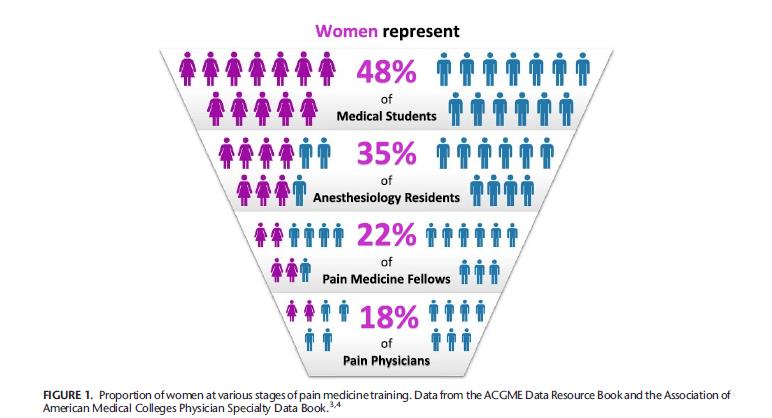
Similarly, while a 2017 survey by athenahealth found that more than 60% of physicians under the age of 35 were women[9], signaling a coming gender shift in healthcare, men still make up more than 63% of physicians overall[10]. In pain specialties, women are severely underrepresented, making up just 26% of anesthesiologists, 19% of pain medicine specialists, and 9.3% of neurosurgeons.[11] The situation is beginning to improve, with women representing 48% of medical students and 35% of anesthesiology residents, but they still represent only 22% of pain medicine fellow trainees.[12]
Figure 1 (Source: Doshi TL, Bicket MC. Why Aren’t There More Female Pain Medicine Physicians?[13])
There is also a large economic gap between those who go into medical school and the general population. While the financial background specific to physicians who opt for pain specialties is not readily available, in looking at all first-year U.S. medical students, 24% came from families that were among the top 5% of earners and 51% came from the top quintile.[14] Meanwhile, only 5% came from the bottom quintile.[15]
This lack of representation matters, not only because—for example—it can be easier for a woman to understand the issues associated with childbirth or chronic pelvic pain, but because the socioeconomic and demographic traits of medical professionals have been correlated with bias,[16] and bias can impact patient assessment, treatment and outcomes[17],[18]
Getting to the Root of the Pain Problem
The second area to look to is the patient perspective. We know that in the U.S., there continues to be significant barriers to care, and if a patient can’t access basic healthcare, then specialty pain care is unlikely to occur. While several issues can contribute to this, some of the most significant are poverty, the educational divide and medical deserts.
Poverty, of course, is chief among these. Wealth inequality has a vast impact on a person’s health. A December 2017 study found that middle-aged Americans who are in the lowest income brackets had a 17% chance of dying compared to just 5% among those in the highest income brackets.[19] Similarly, those with the lowest incomes had a 48% chance of becoming disabled over the next decade while those at the top had only a 15% chance.[20] This same pattern has been demonstrated in patients with chronic pain, who are not only more likely to belong to a lower socioeconomic status[21] but also report feeling pain when faced with economic hardships.[22]
Unfortunately, people with lower levels of income are also more likely to be without health insurance, which can further impede access to care. We know, for example, that even after the implementation of the Affordable Care Act, almost 30 million non-elderly Americans were still without health insurance coverage in 2019.[23] Of those, 1 in 5 made less than the federal poverty threshold.[24]
Without insurance, people are more likely to sacrifice necessary care, including for their chronic pain.[25] As one example, one study found that white male patients with private insurance were more likely to have access to spinal cord stimulators to treat their pain.[26]
Related Content:
In the Face of a Medicaid Tsunami, Telehealth is More Important Than Ever
IoT for Seniors that Promote Health, Autonomy, and Social Inclusion
By the same token, education has been correlated with overall health, as well as with chronic pain. Adults with lower levels of education were more likely to report worse health, regardless of race or gender.[27] National Health Interview Surveys have shown that white men and women had a 57% chance of reporting fair or poor health when they did not have a high school diploma, but only a 9% chance when they had a college diploma.[28] People with less education were also more likely than those with higher levels of education to suffer from non-specific low back pain.[29] Interestingly, people with lower education levels also appear to experience and report more pain with each successive generation that is born—a pattern that is not found in people with bachelor’s degrees.[30]
But all these factors assume people can access the care they need, and for a significant number of Americans, that’s not possible because they live in so-called medical deserts. Often found in rural areas where hospitals have closed and healthcare providers have moved away[31], medical deserts are defined as areas with inadequate access to basic medical services.[32] This forces people to drive longer distances to access care and makes it more difficult for people to access both primary care and specialty care for chronic pain.[33] Ultimately, the need to travel long distances for care has the greatest impact on senior citizens—among those most likely to suffer from chronic pain[34]—and low-income individuals because these groups often face transportation challenges. Without an alternative, these patients are more likely to put off or forego much-needed care.[35]
Digital Health: A Potential Solution
Digital and telehealth are potential solutions for many, helping bridge the divide for those who have few options because of socioeconomic factors. Not only can digital health approaches improve outcomes, but it can also improve mortality, compliance and quality of life.[36] And it can help reduce overall healthcare spending as use of digital health has been associated with cost savings of up to $121 per visit[37], which is a significant reduction for those struggling to pay for their care. But more than that, it can help close the distance between patients and their primary care or specialty physicians. Recent innovations in virtual clinic technology are even allowing interventional pain specialists to make adjustments to neurostimulation devices in patients dealing with chronic pain—a first-of-its-kind advancement in the U.S.
But even as we make advancements, we must continue to find and fill the gaps in care. Digital health, for example, is only as good as the WiFi or computer access at a patient’s disposal. Limited or spotty cell services, slow internet services, and lack of adequate computer technology can keep people from benefiting from digital health options, especially those who are poor in both rural and urban areas.
It is incumbent on all of us—from the healthcare provider to the manufacturer, from payor to policymaker—to break down these barriers to care for all Americans. But to do that, we must first understand the challenges faced in achieving their best health. Only then can we help them restore their health.
References
[1] Mossey JM. Defining racial and ethnic disparities in pain management. Clin Orthop Relat Res. 2011;469(7):1859-1870. doi:10.1007/s11999-011-1770-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3111792/
[2] Samulowitz A, Gremyr I, Eriksson E, Hensing G. “Brave Men” and “Emotional Women”: A Theory-Guided Literature Review on Gender Bias in Health Care and Gendered Norms towards Patients with Chronic Pain. Pain Res Manag. 2018;2018:6358624. Published 2018 Feb 25. doi:10.1155/2018/6358624 .https://pubmed.ncbi.nlm.nih.gov/21249483/
[3] Association fo American Medical Colleges. Diversity in Medicine: Facts and Figures 2019. https://www.aamc.org/data-reports/workforce/interactive-data/figure-18-percentage-all-active-physicians-race/ethnicity-2018. Accessed March 23, 2021.
[4] United States Census Bureau. QuickFacts United States. https://www.census.gov/quickfacts/fact/table/US/PST045219. Accessed March 23, 2021.
[5] Association of American Medical Colleges. Diversity in Medicine: Facts and Figures 2019. Table 12. Practice Specialty, Females by Race/Ethnicity, 2018. https://www.aamc.org/data-reports/workforce/data/table-12-practice-specialty-females-race/ethnicity-2018. Accessed April 27, 2021.
[6] Association of American Medical Colleges. Diversity in Medicine: Facts and Figures 2019. Table 12. Practice Specialty, Males by Race/Ethnicity, 2018. https://www.aamc.org/data-reports/workforce/data/table-13-practice-specialty-males-race/ethnicity-2018. Accessed April 27, 2021.
[7] Association of American Medical Colleges. Diversity in Medicine: Facts and Figures 2019. Table 12. Practice Specialty, Females by Race/Ethnicity, 2018. https://www.aamc.org/data-reports/workforce/data/table-12-practice-specialty-females-race/ethnicity-2018. Accessed April 27, 2021.
[8] Association of American Medical Colleges. Diversity in Medicine: Facts and Figures 2019. Table 12. Practice Specialty, Males by Race/Ethnicity, 2018. https://www.aamc.org/data-reports/workforce/data/table-13-practice-specialty-males-race/ethnicity-2018. Accessed April 27, 2021.
[9] AthenaHealth. The healthcare future is female. . Published Feb. 14, 2018. Accessed March 23, 2021.
[10] Association of American Medical Colleges. Physician Data Specialty Report. Active Physicians by Sex and Specialty, 2019. https://www.aamc.org/data-reports/workforce/interactive-data/active-physicians-sex-and-specialty-2019. Accessed March 23, 2021.
[11] Association of American Medical Colleges. Physician Data Specialty Report. Active Physicians by Sex and Specialty, 2019. https://www.aamc.org/data-reports/workforce/interactive-data/active-physicians-sex-and-specialty-2019. Accessed March 23, 2021.
[12] Doshi TL, Bicket MC. Why Aren’t There More Female Pain Medicine Physicians? Reg Anesth Pain Med. 2018 Jul;43(5):516-520. doi: 10.1097/AAP.0000000000000774. PMID: 29634520; PMCID: PMC6459683. https://pubmed.ncbi.nlm.nih.gov/29634520/
[13] Doshi TL, Bicket MC. Why Aren’t There More Female Pain Medicine Physicians? Reg Anesth Pain Med. 2018 Jul;43(5):516-520. doi: 10.1097/AAP.0000000000000774. PMID: 29634520; PMCID: PMC6459683. https://pubmed.ncbi.nlm.nih.gov/29634520/
[14] Association of American Medical Colleges. Analysis in Brief. An Updated Look at the Economic Diversity of U.S. Medical Students. https://www.aamc.org/media/9596/download. Published October 2018. Accessed March 23, 2021.
[15] Association of American Medical Colleges. Analysis in Brief. An Updated Look at the Economic Diversity of U.S. Medical Students. https://www.aamc.org/media/9596/download. Published October 2018. Accessed March 23, 2021.
[16] FitzGerald C, Hurst S. Implicit bias in healthcare professionals: a systematic review. BMC Med Ethics. 2017;18(1):19. Published 2017 Mar 1. doi:10.1186/s12910-017-0179-8. https://pubmed.ncbi.nlm.nih.gov/28249596/
[17] William J. Hall et al. “Implicit Racial/Ethnic Bias Among Health Care Professionals and Its Influence on Health Care Outcomes: A Systematic Review”, American Journal of Public Health 105, no. 12 (December 1, 2015): pp. e60-e76. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4638275/
[18] Santoro TN, Santoro JD (December 14, 2018) Racial Bias in the US Opioid Epidemic: A Review of the History of Systemic Bias and Implications for Care. Cureus 10(12): e3733. doi:10.7759/cureus.3733. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6384031/
[19] Makaroun LK, Brown RT, Diaz-Ramirez LG, et al. Wealth-Associated Disparities in Death and Disability in the United States and England. JAMA Intern Med. 2017;177(12):1745–1753. doi:10.1001/jamainternmed.2017.3903. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2659324
[20] Makaroun LK, Brown RT, Diaz-Ramirez LG, et al. Wealth-Associated Disparities in Death and Disability in the United States and England. JAMA Intern Med. 2017;177(12):1745–1753. doi:10.1001/jamainternmed.2017.3903. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2659324
[21] Poleshuck EL, Green CR. Socioeconomic disadvantage and pain. Pain. 2008;136(3):235-238. doi:10.1016/j.pain.2008.04.003. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2488390/
[22] Rios R, Zautra AJ. Socioeconomic disparities in pain: the role of economic hardship and daily financial worry. Health Psychol. 2011;30(1):58-66. doi:10.1037/a0022025. https://pubmed.ncbi.nlm.nih.gov/21299295/
[23] Tolbert J, Orgera K, Damico A. Key Facts about the Uninsured Population. Kaiser Family Foundation. https://www.kff.org/uninsured/issue-brief/key-facts-about-the-uninsured-population/. Published Nov. 6, 2020. Accessed March 23, 2021.
[24] Tolbert J, Orgera K, Damico A. Key Facts about the Uninsured Population. Kaiser Family Foundation. https://www.kff.org/uninsured/issue-brief/key-facts-about-the-uninsured-population/. Published Nov. 6, 2020. Accessed March 23, 2021.
[25] Kennedy J, Morgan S. A cross-national study of prescription nonadherence due to cost: data from the joint Canada-United States survey of health. Clin Ther. 2006;28:1217–1224 https://www.sciencedirect.com/science/article/abs/pii/S0149291806001718
[26] Missios S, Rahmani R, Bekelis K. Spinal cord stimulators: socioeconomic disparities in four US states. Neuromodulation. 2014 Jul;17(5):451-5; discussion 455-6. doi: 10.1111/ner.12101. Epub 2013 Aug 7. PMID: 23924155. https://pubmed.ncbi.nlm.nih.gov/23924155/
[27] Zajacova A, Lawrence EM. The Relationship Between Education and Health: Reducing Disparities Through a Contextual Approach. Annu. Rev. Public Health. 2018. 39:273-89. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5880718/
[28] Zajacova A, Lawrence EM. The Relationship Between Education and Health: Reducing Disparities Through a Contextual Approach. Annu. Rev. Public Health. 2018. 39:273-89. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5880718/
[29] Batista, Alexandre Apolinário de Souza, Henschke, Nicholas, & Oliveira, Vinícius Cunha. (2017). Prevalence of low back pain in different educational levels: a systematic review. Fisioterapia em Movimento, 30(Suppl. 1), 351-361. https://doi.org/10.1590/1980-5918.030.s01.ar04.
[30] Case A, Deaton A, Stone AA. Decoding the mystery of American pain reveals a warning for the future. Proc Natl Acad Sci U S A. 2020 Oct 6;117(40):24785-24789. doi: 10.1073/pnas.2012350117. Epub 2020 Sep 21. PMID: 32958666; PMCID: PMC7547221.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7547221/
[31] Schulte A, Majerol M, Nadler J. Narrowing the rural-urban health divide. Deloitte. https://www2.deloitte.com/us/en/insights/industry/public-sector/virtual-health-telemedicine-rural-areas.html. Published Nov. 27, 2019. Accessed Feb. 15, 2021.
[32] Chevillard, Guillaume; Lucas-Gabrielli, Véronique; Mousquès, Julien (2018). Dill, Lan (ed.). “Medical deserts in France: Current state of research and future trends”. L’Espace Géographique. 47: 362–380.
[33] https://www.kff.org/report-section/a-look-at-rural-hospital-closures-and-implications-for-access-to-care-three-case-studies-issue-brief/
[34] NCHS Data Brief. Chronic Pain and High-impact Chronic Pain Among U.S. Adults, 2019. U.S. Centers for Disease Control and Prevention. https://www.cdc.gov/nchs/data/databriefs/db390-H.pdf. Published November 2020. Accessed April 27, 2021.
[35] Schulte A, Majerol M, Nadler J. Narrowing the rural-urban health divide. Deloitte. https://www2.deloitte.com/us/en/insights/industry/public-sector/virtual-health-telemedicine-rural-areas.html. Published Nov. 27, 2019. Accessed Feb. 15, 2021.
[36] Schulte A, Majerol M, Nadler J. Narrowing the rural-urban health divide. Deloitte. https://www2.deloitte.com/us/en/insights/industry/public-sector/virtual-health-telemedicine-rural-areas.html. Published Nov. 27, 2019. Accessed Feb. 15, 2021.
[37] Schulte A, Majerol M, Nadler J. Narrowing the rural-urban health divide. Deloitte. https://www2.deloitte.com/us/en/insights/industry/public-sector/virtual-health-telemedicine-rural-areas.html. Published Nov. 27, 2019. Accessed Feb. 15, 2021.
Allen W. Burton, M.D.
Website:
https://www.abbott.com/
Allen W. Burton, M.D. obtained his Bachelor of Science at the University of Notre Dame, Medical Doctorate at Baylor College of Medicine, and completed his residency at Brigham and Women’s Hospital, Harvard Medical School. He is a board-certified anesthesiologist with an added certification in pain management.
Dr. Burton joined Abbott in October 2015 and served as principal investigator for the ACCURATE and SUNBURST clinical trials bringing 20 years of experience in patient care, alongside a strong background leading large-scale clinical research programs.
He is currently the Medical Director of Abbott’s neuromodulation business, inclusive of Abbott’s neurostimulation and chronic pain management product portfolios.
Prior to joining Abbott, he served as Chairman of the Department of Pain Medicine at the University of Texas MD Anderson Cancer Center from 2000-2011. From 2011-2015, Dr. Burton practiced privately with Houston Pain Associates, where he directed clinical research and participated in many clinical trials.
Dr. Burton’s areas of expertise include chronic pain, pain management, non-opioid alternatives, spinal cord stimulation, dorsal root ganglion stimulation, neurostimulation, and radiofrequency ablation.
He has published more than 50 peer-reviewed articles and authored two textbooks, taught and lectured nationally and internationally, and played an active leadership role among numerous pain societies and editorial boards.


{kind=link}