

How does being insured affect health outcomes? This is a difficult question to answer, partly because of adverse selection (e.g. sicker patients may choose to be insured). But even in the absence of adverse selection, the ability of insurers and uninsured people to diagnose disease may differ.Consider this example Kaliski (2023):
For example, better testing could improve the detection rate of SARS-COV2 infection. If we naively compare the infection death rates of insured individuals to those of the uninsured, we overestimate the impact of having access to insurance. This is because uninsured individuals will detect fewer SARS-COV2 cases, artificially shrinking the denominator when dividing deaths by cases.
The paper goes on to help limit any bias due to differences in diagnostic rates between the insured and the uninsured.The authors use a monotonicity assumption similar to that used in Mansky and Pepper (2000), as long as the direction of any selection bias is known. The two key monotonicity assumptions are:
- monotone subgroup selection. In this case, it means that any given individual is at least as likely to be diagnosed with a disease if they have insurance than if they are uninsured. Very reasonable.
- monotonous diagnostic response. This assumption means that anyone diagnosed with the disease has at least as good an outcome as someone who is not diagnosed. As long as doctors don’t actively harm patients after diagnosis, this is true…again, very plausible.
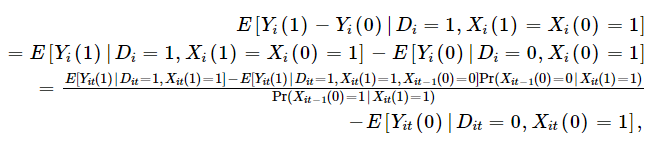
One implication is that those affected by the effect of insurance on outcome are the weighted sum of the effect of insurance on outcome among those who were always diagnosed with or without insurance [Xi(1)=Xi(0)=1] Those diagnosed only through insurance [Xi(1)=1; Xi(0)=0]. Benefits for the insured are weakly limited by the outcome of the insured, since insurance may result in treatment and increase your likelihood of being diagnosed, and the insured will only be diagnosed if they have insurance. Mathematical description using the following monotonic diagnostic response assumption:
Furthermore, if we combine this with the monotonic subgroup selection assumption, Kaliski shows that the “diagnostic constant” subgroup-specific treatment effect of treatment on treated subjects is at least as large as the sample estimate of the subgroup-specific treatment effect.

Kaliski also noted that if the data being analyzed represent the average outcome of undiagnosed (i.e., uninsured) patients in the control group, but diagnosed in the treatment group, then one can determine the effect of treatment unchanged by the diagnosis by assuming :
- (i) persons who would belong to the subgroup of interest, whether receiving treatment or not, or
- (ii) Newly diagnosed patients are not selected on the basis of specific temporal trends when receiving the treatment leading to their new diagnosis.
Mathematically this is:

One can then essentially adjust the observed results among the insured by the likelihood that the diagnosed insured person was not diagnosed before they had insurance. This application requires panel data, but if you have panel data, it can be calculated as follows:
Kaliski then applied this approach to examine the impact of insurance coverage for diabetic insulin therapy on outcomes. As expected, the exogenous change in the likelihood of insurance is the transition to health insurance when people turn 65. Kaliski uses HRS data, which has a panel structure that allows one to examine how diagnosis rates change before and after the transition from commercial/Medicaid to Medicare/other insurance or uninsured. Using this method, he found that:
Using standard staggered difference estimates, and ignoring the effect of new diagnoses, I found that there was a 3% increase in the proportion of people with diabetes who were 65 years of age who started insulin between 2006 and 2009 compared to those who were 65 years of age in 1998 – 2005 . Considering the increase in the number of diabetes diagnoses at age 65 between 2006 and 2009 (Geruso and Layton, 2020), I find that for people diagnosed before age 65, the true effect is likely to be at least as large as the point estimate; 0.6%, relatively speaking, 20% higher.
In short, the rate of insulin use is only 3% comparing the insured to the non-insured, but the real figure should be 3.6%, because Medicare insurance not only allows more diagnosed people to receive treatment, but also allows More people receive treatment. Diagnosed with diabetes and treated for it.
The full text can be read here.


{kind=link}