

There has been some controversy over co-pay cards. These cards or coupons are used to help patients pay for co-payments and deductibles that patients owe when using their medicines. On the one hand, these programs are very beneficial to patients. Some studies have found that out-of-pocket costs for patients have risen dramatically in recent years. For example, in 2009 only 7% of workers had a deductible of $2,000 or more, whereas now 32% of workers have such a high deductible. Payers, on the other hand, claim that co-pay cards increase drug use, which increases medical costs.
To address this, payers have begun implementing co-payment adjustment programs (CAP), such as
Copay Accumulator and Copay Maximizer.
In an accumulator plan, payments made with a self-pay card do not count toward the patient’s deductible or OOP [out-of-pocket] cost max. As such, these plans may increase the overall cost-sharing burden for patients and may result in unexpectedly large mid-year costs.
In a maximization plan, the total annual benefit is allowed to increase up to the maximum amount that the manufacturer is willing to reimburse the patient for out-of-pocket expenses. This amount will be distributed over the patient’s benefit year to balance the use of these available funds. These maximizing plans still do not count toward a patient’s deductible or OOP cost ceiling in a given year, and may delay a patient’s ability to reach this benefit threshold, exposing the patient to further costs related to other medications or illnesses.
An important question is whether (i) co-pay card use differs by racial and ethnic group, and (ii) whether CAP programs differ by racial and ethnic group.This is exactly the research question Ingham et al. (2023) aims to answer. The authors used 2019-2021 data from IQVIA Longitudinal Access and Adjudication Data (LAAD) to perform a 1:1 match with Experian Marketing Solutions, LLC consumer data. The former is a claims data source and the latter is a consumer data source. Using these data files, the authors found that:
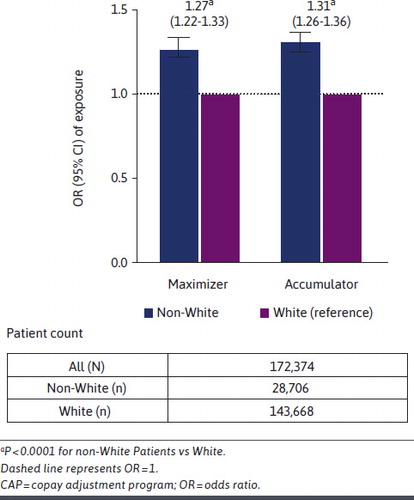
…the rate of copay card use was not significantly different between nonwhite and white patients (odds ratio [OR] = 0.995, 95% CI = 0.99-1.00; phosphorus = 0.0964). However, among co-pay card users, non-white patients were significantly more likely to be exposed to CAP, as maximizers (OR = 1.27, 95% CI = 1.22-1.33; phosphorus < 0.0001) or accumulator (OR = 1.31, 95% CI = 1.26-1.36; phosphorus < 0.0001), compared with white patients.
full article available here.


{kind=link}