

In 2020, specialty drug spending was $265 billion; this constitutes 49.6% Total spending on prescription drugs. In response to rising costs, payers have turned to white, brown and clear bags and care settings that restrict patients from receiving specific medications. What are these “bagging” policies, what are the pros and cons, and what legislation has been passed or is being considered to limit the ability of payers to implement these programs. Today, I summarize a white paper from ICER titled “White Bagging, Brown Bagging, and Service Site Policies: Best Practices for Addressing Provider Markups in the Commercial Insurance Marketplace“. This post follows my previous post topic two years ago.
definition
- white bagging A policy to ship medications from a specialty pharmacy directly to the provider at the point of service (usually a doctor’s office, HOPD, or home infusion provider) where the medication will be administered. The provider is responsible for receiving the medication from the specialty pharmacy, unboxing it, and storing it until the patient arrives on-site and ready to be administered. The nickname “white bagging” comes from the “white coats” of providers who receive medications from specialty pharmacies. Analysis of the impact of white bagging on payers and patients is discussed later in this article.
- brown bagging The policy requires patients to pick up clinician-prescribed medications at a specialty pharmacy, or to have these medications delivered directly to the patient, after which the patient is responsible for storing these medications until their clinician appointment, when the patient takes their medications with them to deliver Managed by clinicians. The term “brown bag” comes from the analogy of the “brown bag” lunch that individuals carry.
- clear bagging Involves the provider, usually the hospital, to create a formal process by which its in-house specialty pharmacy dispenses the drug and ships it to the point of service. Hence, clear bags serve as a supplier strategy to provide an alternative to white and brown bags, thereby preserving revenue associated with specialty drug delivery. Clear bagging also avoids some of the logistical and safety challenges associated with white bagging. For example, if a patient’s medication dose needs to be adjusted, a hospital specialty pharmacy can dispense a new dose and deliver it to an on-site hospital suite or clinic without having to reschedule a patient’s appointment like white bagging. Hospital-owned specialty pharmacies have proliferated recently, according to 2019 Estimates for 2010 show that 26% of hospitals have specialty pharmacies.
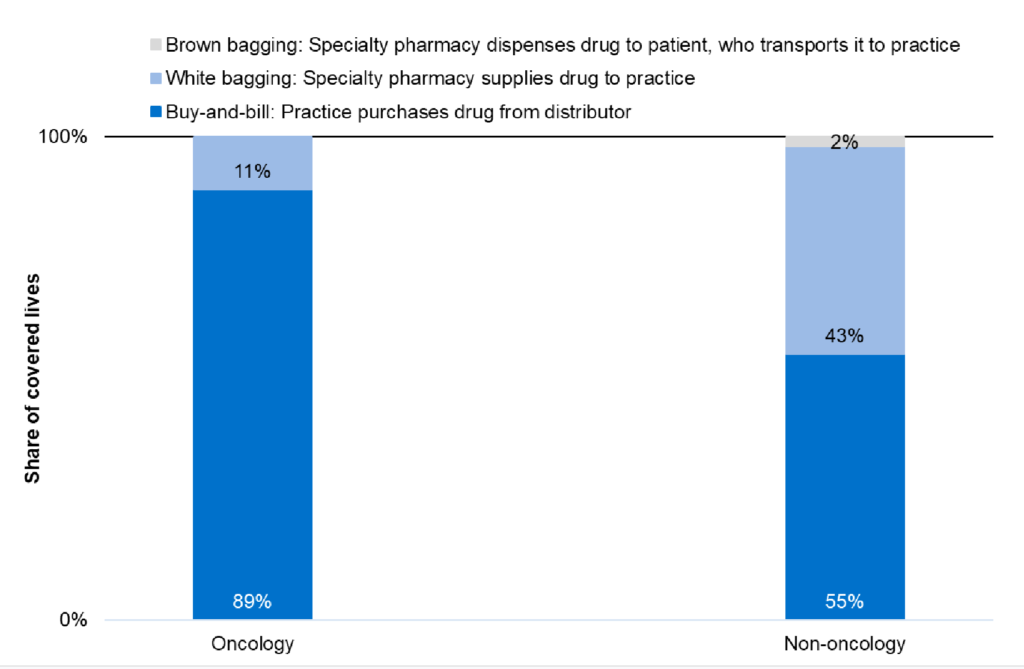
How common are these practices? So, starting in 2022, 27% of oncology products Administration in a physician’s office under commercial insurance is subject to a white bag policy. This is partly driven by industry consolidation.
It is more common in non-oncology products, as shown below in the data through 2019.
Part of the reason for the increase in “bagging” policies has to do with industry consolidation.
The top three PBMs aligned with payers — CVS/Aetna, Optum/UnitedHealthcare and Express Scripts/Cigna — accounted for 77% of all prescription drug claims. 36,37 Some providers assert that the bagging policy is motivated by health plans wishing to drive volume to their own specialty pharmacies.
Place-of-service restrictions aimed at diverting patients to lower-cost care settings are also becoming more common. According to a survey:
…by 2020, almost 70% of business plans will have an onsite service program, with 34% mandatory and 32% voluntary. 24 The same survey found that commercial payers had shifted 30 percent of all field service strategies in 2019, with 19 percent of members going into home infusions, 19 percent going to outpatient infusion rooms, and 14 percent going to independent physician offices.
The main criticisms of white and brown bagging are:
- patient safety. Especially with brown bag packs, patients may not be able to properly administer these particular medications at home. Also, due to long travel times, medications may spoil if not properly refrigerated.
- Impact on Vulnerable Patients. For patients with limited transportation options, brown bagging can be burdensome for the patient.
- Incorrect prescription, difficult to change prescription. In one survey, 66% of respondents indicated that the products they received in white packaging were no longer correct due to newer regimens or dosage changes.
- Patient pays out of pocket. Lower payer costs from white and brown bagging are generally not passed on to patients. In fact, OOP costs may increase if the drug is moved from being part of the medical (ie, physician-administered) benefit to the patient’s pharmacy benefit.
- supplier revenue. Providers – especially 340B hospitals – could experience significant revenue loss as drug administration moves from hospital pharmacies to payer-owned/controlled specialty pharmacies.
- drug waste“Because medications obtained in white or brown bags are for the individual, rather than the purchasing and billing process where physicians purchase the medication to keep in stock, any excess medication in the white or brown bag vial must be discarded and cannot be used. For another patient, make the payer and patient responsible for the entire vial and associated cost-sharing.”
Likewise, criticisms of service location restrictions include: (i) increased patient travel burden, (ii) reduced oversight of adverse event monitoring, and (iii) negative impact on provider (particularly hospital outpatient facilities) revenues.
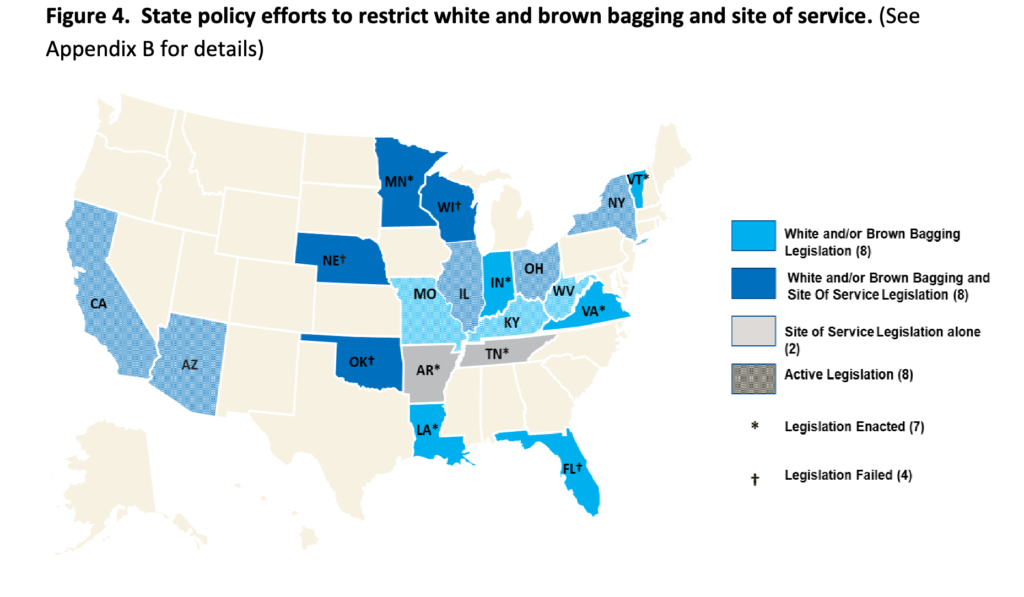
Legislative initiatives.
- white bagging: Three states (Los Angeles, Minnesota, Vermont) have passed legislation restricting white bagging, and nine states (Arizona, California, Illinois, Kentucky, Missouri, New York, Ohio, West Virginia) Legislation has been proposed to limit payer-mandated white bagging
- brown bagging. Two states (Virginia and Vermont) have implemented policies banning brown bagging.Proposed legislation in three states (California, Illinois, New York) would ban brown sacks in addition to white sacks
- service point. Three states (Arkansas, Minnesota, Tennessee) have passed legislation prohibiting payers from requiring home infusions of clinician-administered medications.


{kind=link}