

My mission as Doc Gumshoe is almost the contrary of what the mainstream media do every day. They give prominence to disasters – a train wreck, an earthquake, an outbreak of a dire disease – which get promoted to the top of the news. Doc Gumshoe deals in an area which is fundamentally not cheerful and pleasant. If we all lived in perfect health until our number came up and we were easily transported to whatever lies beyond, there would be no need for healthcare and no role for Doc Gumshoe. But the reality, unfortunately, is quite different.
In the context of that reality in which we all live, I take it upon myself, in combing through the information that comes into my orbit just about every hour, to find the optimistic bits. But that doesn’t mean that I squelch the relevant bad news. I don’t pay much attention, for example, to failed drug clinical trials, of which there seem to be a constant stream.
However, one potentially gigantic lawsuit is looming, based on news that could only be considered as definitely bad. Seventy thousand people are suing GlaxoSmithKline (GSK) because one of their lead pharmaceuticals, Zantac (ranitidine) can, in certain circumstances, form a potent carcinogenic substance, usually called NDMA. That stands for nitrosoldimethylamine, less than a milligram of which can mutate mice cells. Two grams can kill a human in a couple of days. NDMA is one of a group of chemicals called nitrosamines, all of which are carcinogenic. Nitrosamines can actually form in the stomach when nitrites, which are found in such comestibles as grilled and smoked meats, combine with amines, which are present in many medications. Small amounts are unlikely to do significant harm, but it would certainly seem like a best practice to limit the amounts of nitrosamines in one’s system. Many people, including my own spouse, scrupulously avoid nitrites.
The news that Zantac could be tainted with high levels of probable carcinogen became public in 2019. Health regulators around the world withdrew approval, and in the spring of 2020 the FDA forced Zantac off the market in the US. Since then, no US company can manufacture ranitidine.
At this time there doesn’t seem to be any evidence that taking Zantac has actually caused a case of cancer in any person, although it would be difficult to prove that a particular case of cancer in a person who regularly took Zantac was in fact due to Zantac. The grounds for the lawsuit are that GSK has known about the formation of NDMA in their drug for something like 40 years and withheld that knowledge from the general public.
Doc Gumshoe is not a lawyer, but it seems to him (me!) that it would be difficult to prove in a court of law that taking Zantac actually caused any harm to the 70,000 plaintiffs in those prospective lawsuits. And by the way, both Pfizer and Sanofi have also sold Zantac and are therefore party to those lawsuits. But even if GSK and the others are not found liable for harms to those plaintiffs, they are apt to suffer reputational damage, which could hurt them as they develop and promote other pharmaceuticals. I would not be surprised if there were a considerable settlement.
However, returning to my fundamental mission, here are several bits of news that are definitely optimistic.
Slow, but real progress in countering the effects of Alzheimer’s disease
The news of the day is that the US Veteran’s Administration announced that it will cover prescribing Leqembi (lecanemab) to qualifying US veterans with early stage Alzheimer’s. The VA will cover any veteran who meets certain criteria, including an MRI scan within the previous year, amyloid PET imaging consistent with Alzheimer’s, and a test indicating mild Alzheimer’s dementia. This follows the FDA granting accelerated approval to Leqembi in January of this year. There is some expectation that full FDA approval of Leqembi will take place before the end of March. Leqembi was developed by Eisai and will be marketed by Biogen.
Leqembi’s accelerated approval was based on preliminary evidence that lecanemab eliminates toxic amyloid beta (Aβ). However, in this case Eisai is expected very shortly to submit the data on improved cognition to the FDA, which will then consider the drug for full final approval. Eisai has reported early results from a large clinical trial in which Leqembi/lecanemab slowed both cognitive and functional decline in patients with early-stage Alzheimer’s by 27% compared with placebo subjects.
An adverse effect of concern is brain bleeding, which has resulted in the deaths of two patients thus far. Those two patients were taking blood thinners, which considerably increases the risk of a brain bleed. In patients not on blood thinners the risk is very low and manageable according to the investigators.
Lecanemab/Leqembi will be restricted to patients with early stage Alzheimer’s who also have deposits of Aβ in their brains. However, it is the first approved drug that shows significant benefit in the treatment of persons with Alzheimer’s disease. Note, FDA’s limited approval of Aduhelm was based not on clinical efficacy, but on its demonstrated reduction of Aβ deposits.
Lecanemab/Leqembi’s mechanism of action is fundamentally different from that of aducanumab/Aduhelm. Aduhelm removes Aβ deposits from the brain, whereas Leqembi recognizes the fibrils that form Aβ and prevents them from combining into deposits of the amyloid plaque. It is a monoclonal antibody consisting of a humanized version of a mouse antibody that prevents Aβ deposition in animal models of Alzheimer’s disease.
Another drug with the same target has shown definite results in reducing Aβ deposits. The drug is donanemab, from Eli Lilly. Donanemab, also a monoclonal antibody, hit all primary and secondary goals of the six-month primary outcome analysis in the clinical trial, dubbed TRAILBLAZER-ALZ 4. The study enrolled 148 patients with early symptomatic Alzheimer’s, with investigators assessing superiority regarding the percentage of participants who reached complete amyloid plaque clearance at six months, as measured by PET scan. At six months, 37.9% of donanemab-treated participants experienced complete brain amyloid clearance compared to 1.6% of Aduhelm-treated patients, according to the new data. In the study population as a whole, donanemab reduced brain amyloid plaque levels by 65.2% at six months compared to baseline, while Aduhelm reduced levels by 17% for the same time period. Treatment with donanemab not only produced significant reduction of amyloid buildup in the brain, but also of plasma phosphorylated tau (P-tau) in the blood after six months.
What needs to be emphasized about both lecanemab/Leqembi and donanemab is that these agents did not merely reduce the accumulation of amyloid plaque, but removed plaque that had previously accumulated, and in some cases totally cleared the brain of plaque. If indeed plaque is the principal culprit, then these drugs have the potential of actually resolving or curing some cases of Alzheimer’s disease.
Lilly has four other clinical trials with donanemab in progress. Results from a placebo-controlled trial of donanemab’s clinical efficacy and safety are will be reported in the spring of this year. Expectations are high!
A potential vaccine against Alzheimer’s disease?
On January 26th, the Swiss biotech AC Immune announced interim findings from a Phase 1b/2 clinical trial of a prospective vaccine aimed at preventing the formation of amyloid beta. In this clinical trial dubbed ABATE, the candidate agent ACI -24.060 elicited an antibody response to Aβ in the cohort of trial subjects who were given a low dose of the agent. The response was detectable as early as six weeks after dosing. ACI-24.060 was generally well tolerated with no safety concerns observed. Based on these findings, dosing in a second, higher dose Alzheimer’s cohort has begun.
The trial will now be expanded to include subjects with Down syndrome, who also have deposits of Aβ in the brain. Most patients with Down syndrome exhibit Aβ plaques as well as the tau tangles which are characteristic of Alzheimer’s. The company expects to release further immunogenicity data from the study’s cohorts in the second half of 2023. But investors will have to wait until 2024 to find out if ACI-24.060 actually reduces amyloid plaques, which AC Immune intends to measure by PET imaging. What would qualify ACI-24.060 as a vaccine is that it creates polyclonal antibodies that persist in the vaccinated individuals. It is these antibodies that are thought to prevent the formation of Aβ.
It’s early days for that potential Alzheimer’s vaccine, and also for the drugs that we discussed earlier. But regardless how we look at it, the overall picture of Alzheimer’s has changed quite a bit. We have learned that it is possible to detect Alzheimer’s before the most damaging consequences have manifested, and there is good reason to believe that some of the treatment options that have emerged would be effective if instituted earlier in the course of the disease.
It’s not a pipe dream. We’re on the path to effective management of Alzheimer’s!
Optimism is warranted with regard to cancer
“reveal” emails? If not,
just click here…
The American Cancer Society published an article on January 12th entitled “Risk of Dying from Cancer Continues to Drop at an Accelerated Pace.” The statistical basis for this highly positive statement is that in the US there was a 32% drop in the cancer death rate between 1991 and 2019, which translates to about 3.5 million fewer cancer deaths during those years if the fatality rate had continued at the 1991 level. The ACS quickly went on to say that the large reduction in the number of cancer deaths is primarily because of a reduction in the numbers of people smoking, which resulted in major declines in the numbers of lung cancers and other smoking-related cancers.
However, after this modest disclaimer (we in the medical community cannot solely claim credit for saving those lives!), the article goes on to specify three areas where the medical community does deserve credit. These are:
- Chemotherapy after surgery for breast and colon cancer
- Combination therapy for many cancers
- Prevention and/or early detection through screening for some cancers, including cancer in the breast, cervix, colon, prostate, rectum, and more recently, lung.
Chemotherapy has been attacked, in particular by proponents of alternative cancer therapies, who frequently characterize mainstream cancer treatment as “poison, cut, and burn,” for chemotherapy, surgery, and radiation. There is some justification for calling chemotherapy “poison,” because chemotherapy agents do not distinguish between healthy cells and cancer cells, thus normal cells are also damaged along with cancer cells. But cancer cells reproduce much more quickly than normal cells – that’s what accounts for rapid tumor growth, among other things. That also makes them a better target for chemotherapy agents, which can kill them in the process of formation. Most normal cells recover from damage fairly quickly, while cancer cells do not recover.
It’s also the case that there has been a great deal of progress in the development of chemotherapy agents, so that currently these agents are much safer than when the principle of chemotherapy was first introduced.
There are at least six classes of chemotherapy agents, including alkylating agents, antimetabolites, anti-tumor antibiotics, topoisomerase inhibitors, mitotic inhibitors, and corticosteroids. The total number of drugs that could be considered chemotherapy agents is in the hundreds, and cancer specialists choose carefully which of these agents to use, depending on the specific type of cancer, the degree to which it has spread, and factors specific to the patient such as co-morbidities.
Early detection is crucial
Lung cancer
Lung cancer is the leading cause of cancer deaths in both men and women, accounting for 21% of all cancer deaths in the US. The estimated number of lung cancer deaths in 2023 is 67,160 in men and 59,910 in women. That comes to about 350 deaths per day – more than breast, prostate, and pancreatic cancers combined. About 81% of lung cancers are caused by cigarette smoking. Smokers are about 25 times more likely to develop lung cancer than non-smokers.
However, in both men and women, there has been a shift in the diagnosis of lung cancer – a decline in the number of advanced disease diagnoses along with a small (4.5%) increase in the number of localized disease diagnoses. The overall result was a considerable increase in the 3-year survival rates of persons diagnosed with lung cancer. In 2004, 21 out of 100 people were living 3 years after their diagnosis, and in 2018, that number had risen to 31 out of 100 people. It has been pointed out that only in 2013 did the American Cancer Society and the US Preventive Services Task Force (USPSTF) recommend screening for lung cancer. An earlier recommendation might well have resulted in earlier improvements in the 3-year survival rate.
Early detection is only partly responsible for this improvement in lung cancer survival. There have been improvements in the means of diagnosing lung cancer, but also improvements in treatment, such as video-assisted surgery and drugs that specifically target the most common gene mutations in lung cancer.
Prostate cancer
From the mid-1990s to the mid 2010s, the risk of death from prostate cancer decreased by about 50% due to improved treatment and earlier detection by means of prostate antigen (PSA) testing. Since then, the risk of death from prostate cancer is declining by only 0.6% per year despite further improvements in treatment. The cause of this major change in this declining rate is almost certainly the change in screening guidelines. In 2009, the USPSTF recommended against routine PSA testing for all men over age 75, and in 2012 against PSA testing for all men. As a result of the USPSTF’s recommendations, the incidence of more advanced prostate cancer has more than doubled in the past 10 years, from 3.9% to 8.2%. A 2022 study by the University of Southern California’s Keck Medicine also showed that the incidence rate of metastatic prostate cancer rose as much as 43% in men 75 and older and 41% in men 45-74 after routine prostate cancer screenings were no longer recommended.
The ACS reports that after the 2012 USPSTF guidelines, there was a steeper drop in PSA testing in Black men than in White men. It was noted that this is of particular concern, because early detection is especially important in Black men.
And while we’re talking about prostate cancer, there’s recent evidence that the risk is strongly determined by genes, specifically the genes BRCA2, HOXB13, and BRCA1. Looking at a database on 170,000 men who had not developed prostate cancer, researchers found that among 7,600 of those men who developed the cancer over a ten-year period, the researchers found that the majority of the prostate cancer patients could have been identified as moderate to high risk prior to their diagnosis. The percentage of men expected to develop prostate cancer was 54% among those with a BRCA2 gene mutation, 39% for those with the HOXB13 variant, and 17% for those with a BRCA1 mutation, according to the model.
Breast cancer
The incidence of breast cancer in women has been slowly increasing by about 0.5% per year since the mid 2000s. This is largely due to increasing rates of obesity in women, and also to a decline in the birth rate and to the fact that more women are having their first child after age 30 – factors that are statistically linked to increases in the incidence of breast cancer. Mutations in the BRCA1 and BRCA2 genes tend to make cells divide more rapidly, which increases the chances that cells will mutate and become cancerous. About one in every 500 women in the US has a mutation in one or the other of those genes.
Disparities in cancer incidence and survival
The ACA labels the factors that can lead to these disparities as “sociodemographic” and lists them as follows: “race, ethnicity, age, income, sexual orientation, gender identity, or the place where a person lives.” The examples they cite do not, in my opinion, strongly validate their characterization of those factors.
- In 2019, 27% of men without a high-school education smoke cigarettes, compared to 6% of men with a college degree. The ACA asserts that tobacco companies specifically market in neighborhoods where men do not have a college degree.
- Black women have a 4% lower incidence of breast cancer than White women, but a 41% higher death rate.
- American Indians and Alaska Natives have the highest incidence of liver cancer of any major racial or ethnic group in the US, more than double that in White people.
The ACA correctly pointed out that the COVID-19 pandemic had a major impact on the ability of many people to access available services for cancer prevention, especially detection and prevention, and that this impact was not evenly distributed across all sectors of society. Regarding breast cancer screening, the USPSTF backed off on its prior recommendation for mammograms for women under age 50, now stating only that they should discuss it with their doctors. Women 50 to 74 should have a mammogram every two years, according to their more recent recommendations. However, “discuss it with your doctor” assumes that the woman in question has a regular doctor with whom she regularly chats about her health issues. That assumption does not apply across all sectors of society.
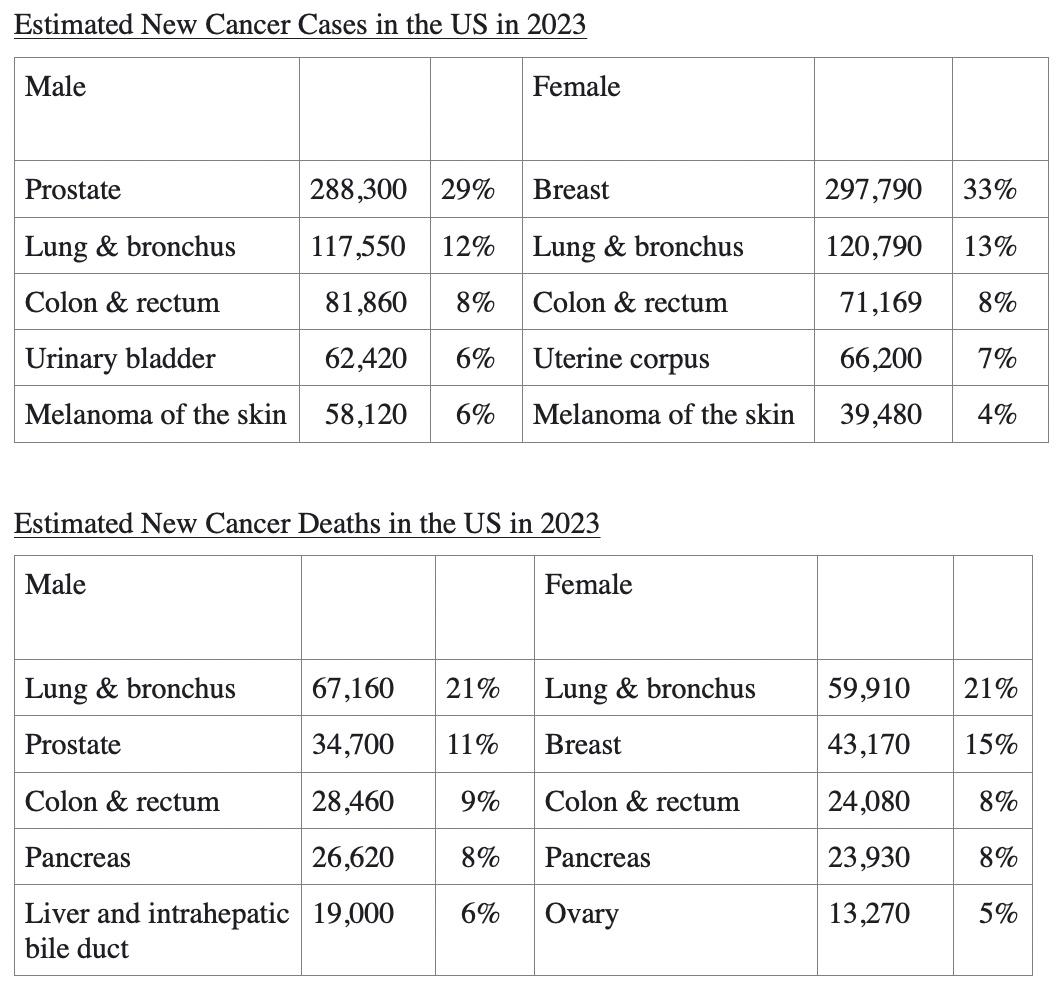
Here’s what the ACA predicts the overall cancer picture will look like:
That’s not the entire picture, of course – there are many other cancers affecting both males and females. But those estimated numbers tell us something for sure. For example, in men prostate cancer is the most common in terms of incidence, but not the leading cause of death – according to those estimates, about 88% of men diagnosed with prostate cancer will survive. And about 85% of women diagnosed with breast cancer will survive. In contrast, pancreatic and liver cancers are not among the most frequent in terms of incidence, but they are predicted to cause 14% of all cancer deaths. The charts above give a quick indication of the predicted impact of cancer in the US.
Advances in cancer treatment
While it’s certainly true that a large part of the decline in cancer cases and cancer deaths is due to factors like a big decrease in cigarette smoking and an improvement in early detection, the pharmaceutical sector has made huge advances in the past and continues to do a great deal of research on that front. The research tends to focus on highly specific forms of cancer – cancers that are associated with certain genetic characteristics, cancers that have recurred after treatment or not responded to treatment, and cancers that have previously been considered extremely resistant to treatment.
Often, the number of individuals who stand to benefit from these treatments is not large, and the reward for pharmaceutical companies doing research on such cancers may look chancy. The pharmas often attach very high price tags to their prospective candidates, hoping to make up in these elevated prices what they will lack in volume of sales.
But what also happens with some regularity is that a drug that receives approval for one specific form of cancer then goes on to win approval in other cancers. The prime example is Merck’s Keytruda, which first gained FDA approval for non-small-cell lung cancer in 2014 and has gone on to score 17 more indications. Keytruda’s 2021 sales were more than $17 billion.
A prospective example of this is Roche’s Tecentriq (atelolizukmab). Roche has just announced positive results in reducing the risk of tumor recurrence in patients with metastatic liver cancer. In combination with the widely-used agent Avastin, Tecentriq reduced tumor recurrence when used as adjuvant treatment after surgery in persons with hepatocellular carcinoma at a high risk of rebound.
This may sound like a very narrow slice of the market to go after, but it could be life-saving treatment for those at risk. Tecentriq is currently approved for bladder cancer, non-small-cell lung cancer, breast cancer, small cell lung cancer, hepatocellular carcinoma, and melanoma. Tecentriq is a monoclonal antibody designed to bind with a protein called PD-L1 expressed on tumor cells and tumor-infiltrating immune cells. By inhibiting PD-L1, Tecentriq may enable the activation of T-cells, which attack tumor cells.
Tecentriq did not do well in a trial in patients whose surgery for liver cancer failed to eliminate the disease, but Roche is optimistic about upcoming trial results in patients after surgery for head and neck cancer, and also in triple-negative breast cancer. (Triple-negative breast cancer means that the cancer cells don’t have estrogen or progesterone receptors and make very little of the HER2 protein. It grows and spreads faster and usually has a worse prognosis.)
Engineering T-cells to attack pancreatic cancer
Pancreatic cancer is one of the most challenging of all cancers. It develops entirely within the pancreas, causes no early symptoms and is therefore exceedingly difficult to detect in the early stages. Even when it does cause symptoms, those are very non-specific – fatigue, loss of appetite, weight loss, and in some cases jaundice. And treatment options for pancreatic cancer have been very limited, such as surgical removal of the entire pancreas. Radiation which targets only the tumor within the pancreas can be attempted, but the success rate is not high. Only 11% of patients who have been diagnosed with pancreatic cancer survive five years after diagnosis.
In this context, researchers at the University of California San Francisco (UCSF) have developed a new T cell-based immunotherapy that selectively targets cancer cells.
There were significant obstacles to overcome in order to make it possible for the T-cells to attack and destroy the cancerous tumors. T-cells normally attack cancer cells, but solid tumors build multiple defensive walls that prevent the killer T-cells from entering and destroying the tumors. However, the T-cells engineered by the researchers deliver interleukin 2 (IL-2), a naturally-occurring inflammatory molecule produced by the immune system that has powerful anti-cancer effects. IL-2 supercharges T cells, making them more effective cancer killers. The anti-cancer effects of IL-2 have long been known; however, systemic administration of IL-2 has been limited due to the severe side effects it can cause. Simply infusing patients systemically with IL-2 can cause high fever, leaky blood vessels, and organ failure.
The researchers were able to avoid this problem, which would have prevented the T-cells from doing their job, by programming the tumor-infiltrating T-cells to make their own IL-2 when they recognized a cancer cell. The therapy, employing the engineered T-cells, effectively eliminated both melanoma and pancreatic cancer in mice, with minimal side effects.
The engineered T-cells produce the IL-2 only when they have entered the tumor. To engineer cells that could sense when they were in the tumor, the researchers used a synthetic Notch (or synNotch) receptor, a flexible type of molecular sensor, which had been developed in the UCSF lab several years earlier. These receptors span the cell membrane, with ends that protrude both inside and outside the cell. The outside portion recognizes and binds to tumor cells, triggering the inside portion to set the production of IL-2 in motion.
The circuit begins when the synNotch receptor tells the T-cell to make IL-2. That IL-2 feeds back on the cell, causing it to divide, in turn creating more cells that make even more IL-2. The entire process is confined within the tumor, protecting the rest of the body from harm.
The investigators hope to begin testing the therapeutic approach in clinical trials with pancreatic cancer patients in 2024.
The paper describing the research was published in Science in December, 2022. (Allen G. “Synthetic cytokine circuits that drive T cells into immune-excluded tumors.” DOI: 10.1126/science.aba1624)
These findings are significant in several ways. First, they point to possible treatment options for a form of cancer which has been highly treatment-resistant. But also, they illustrate the ways in which researchers have been able to manipulate T-cells to maximize their disease-treating capacities. And they also demonstrate that it is possible to introduce artificial cytokines into the human body in order to facilitate therapeutic goals.
The possibility of modifying T-cells to treat cancers in specific patients has been a reality for a number of years, but treatment of this sort required tailoring the T-cells to a specific cancer, not just to a class of cancers, and had not been successful in treating solid tumors. The innovation in this study was tailoring the T-cell to release the cancer-killing IL-2 only when it had entered the solid tumor. It was not necessary to tailor the T-cell to the specific tumor. The technique is designed to be effective in solid tumors as a class.
We can look forward to further advances along those lines.
* * * * * * *
I was planning to cover considerably more territory in this installment, but as I got into it, the details of each topic seemed worth exploring. Therefore I will need to continue in this vein in my next piece. There keep being genuinely interesting happenings in this area, and I will pass them along to you. Do please let me know if there are specific subjects you want to know more about. Many thanks and best to all, Michael Jorrin (aka Doc Gumshoe)
[ed note: Michael Jorrin, who I dubbed “Doc Gumshoe” many years ago, is a longtime medical writer (not a doctor) and shares his commentary with Gumshoe readers once or twice a month. He does not generally write about the investment prospects of topics he covers, but has agreed to our trading restrictions. Past Doc Gumshoe columns are available here.]


{kind=link}
{kind=link}